Advanced cardiac MRI and PET in clinical trials
I’ve used 4D flow MRI in clinical studies and trials too, with the end goal of advancing the management of cardiovascular disease.
As part of this work, I’ve worked in collaborative teams of cardiologists, radiologists, scientists, engineers, and biostatisticians to design and execute clinical trials and studies on cardiovascular diseases and interventions using MRI and simultaneous PET/MRI imaging endpoints.
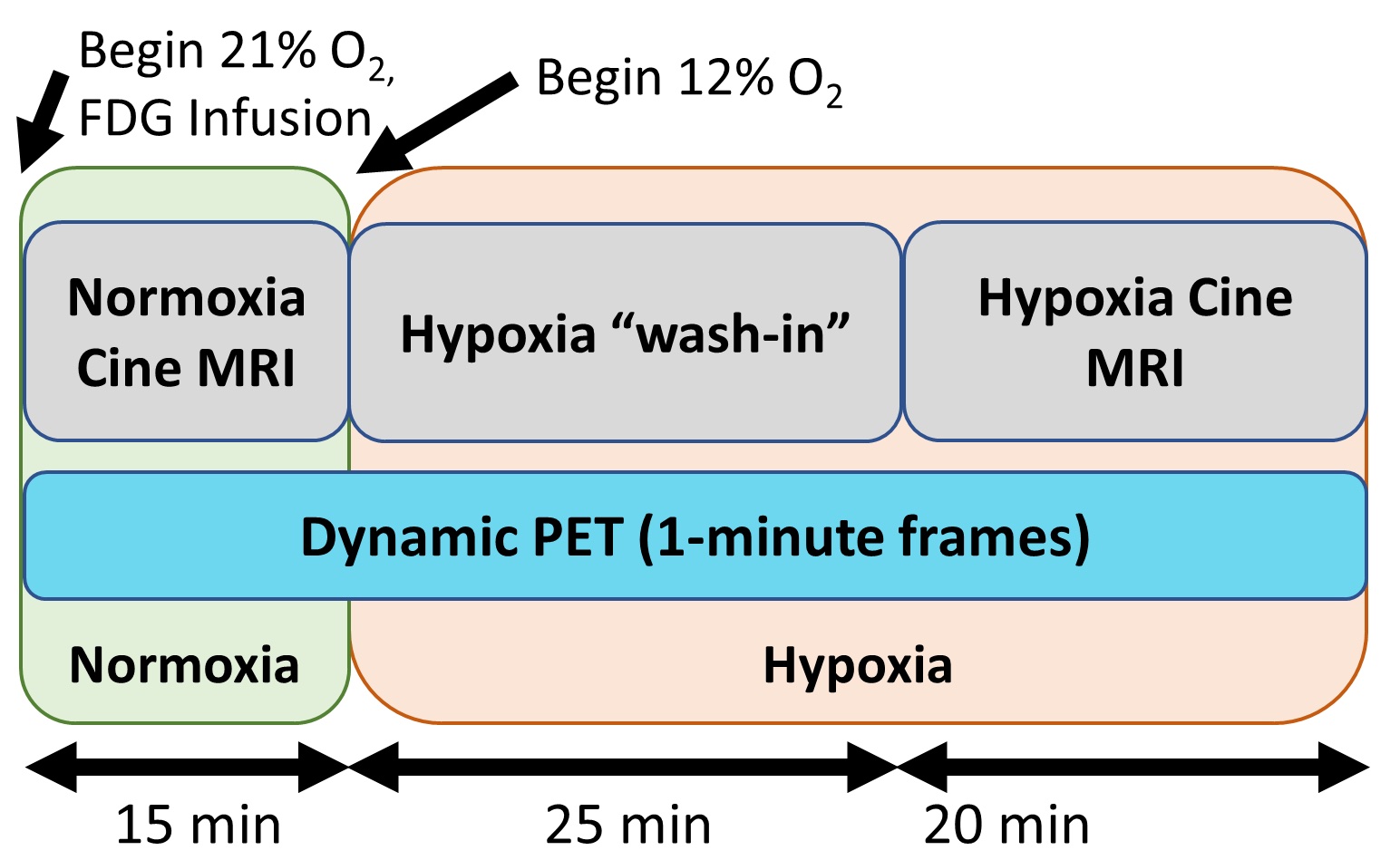
In clinical trials looking to study cardiac physiology in adults born extremely premature, my team is assessing pharmaceutical interventions (NCT03696758 and NCT04090866 on clinicaltrials.gov) and hypoxic gas as a stress test (NCT03245723).
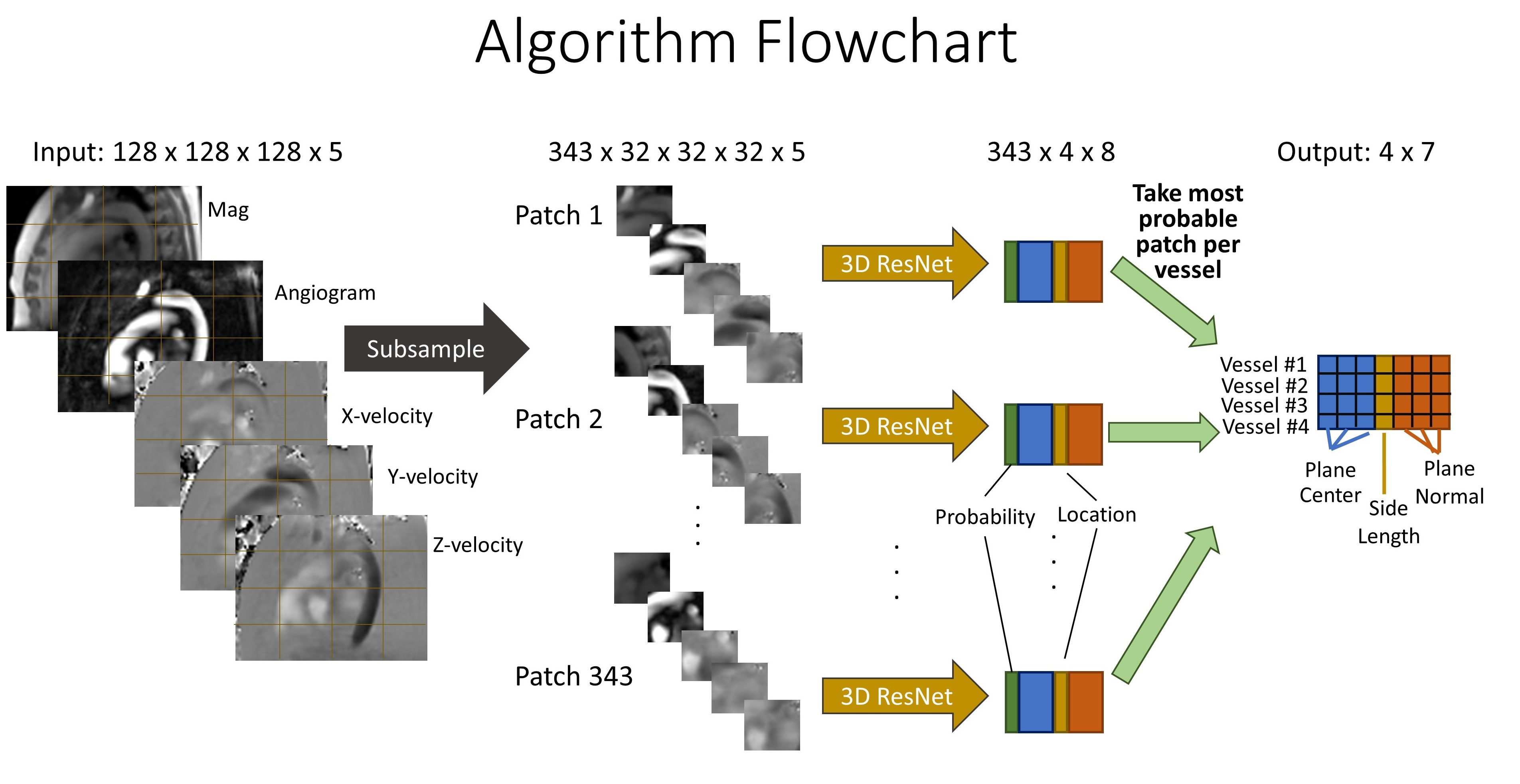
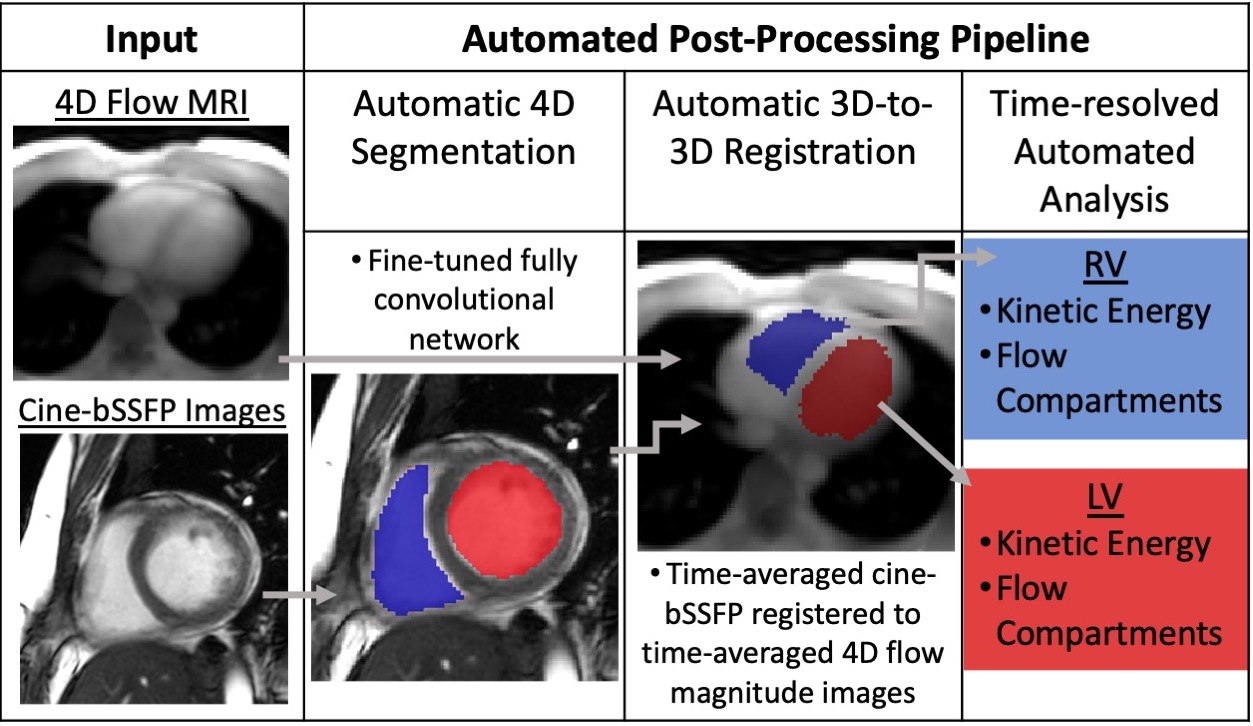
Throughout the projects I’ve taken the lead on image analysis methods for advanced cardiac MR images, writing custom code in Matlab and python to measure imaging biomarkers demonstrated in the literature.
I’ve also led the statistical analysis and interpretation efforts pertaining to these and PET images, with help from clinicians and biostatisticians, resulting in 3 first-authored publications in the late stages of peer-review stemming from these trials.
In the later 2 trials, I’ve also been involved in setting up the imaging protocols including MRI and PET acquisition parameters and data management.